
Orphanisation blog
Blog posts for the Wellcome Trust funded 'Orphan drugs: high prices, access to medicines and the transformation of biopharmaceutical innovation' project.

- World Orphan Drug Congress USA - Boston 2024
-
The Orphanisation team spoke at the World's leading pharmaceutical conference on orphan drugs. Matthew Hanchard discussed the value of social media data for diagnosis and Jin Ding covered growing US-EU disparity between drug submissions and approvals.
Having attended several Terrapin events over the last three years as part of our ongoing ethnography of pharmaceutical conferences - speaking at the World Orphan Drug Congress (WODC) in Boston, USA held a slightly different feel. In Europe, we have covered how the World Evidence and Pricing (EPA) Congress in 2022 and 2023 in previous blog posts - both of which held a strong focus on market access, bringing together industry, patient organisations (POs), and regulators. At the WODC, the focus seemed to flow back to market access, but gravitated too towards finding solutions to core issues like the diagnostic odyssey, the pricing wrangle over orphan drugs, regulatory hurdles left to overcome. Discussion felt polemic. The shift in tone followed into the stalls too, where stands like PCMtrails selling at home testing kits for âdecentralised clinical trialsâ, jostled with various real-world data and consultancy services of all kinds, through to pre-constituted survey panels, and several POâs. Yet curiously, unlike the World EPA Congress, there were no biotech and pharma companies there (big, SME, or startup) to set up shop in the lobby. This made it it a little unclear on who exactly the Clinical Research Organisationsâ (CROsâ) target clients might be! Surely, CROs cannot sell simply to other CROs alone? The conference talks deviated slightly from the World EPA Congress too in their scope of discussion. Rather than a track on âRare Diseaseâ it held one on âRare Oncologyâ. Meanwhile, âMarket Accessâ became âGlobal Market Accessâ, and âBig Data and Digital Healthâ became âAI and Digital Healthâ - subtle but notable differences in framing. The WODC also held a much larger poster session with space for a patient art exhibition, giving attendees time to engage with cutting-edge research, becoming far more of a site for recruitment and headhunting of future staff.

Stalls - World Orphan Drug Congress - Boston 2024

Exhibition - World Orphan Drug Congress - Boston 2024
Beyond surface appearances, the content of discussion at the event also differed from the World EPA Congress. Over the past three years, the World EPA Congress has moved from a post-pandemic concern for maintaining stability and sustainability in the market through increasing access onto a recent focus on addressing policy wrangles around how to ensure patients gain equitable access to orphan drugs (despite their high price). The WODC somehow felt more solution-focussed, with health economists and activists thrashing out new and novel potential ideas; albeit interspersed with very clear sales pitches for products and services. Within this, some sage perspectives came forward. Championing industry, within a panel worryingly titled âMonetising Hopeâ, Patroski Lawson (CEO of KPM Group DC) noted that â...about 75% of innovation comes from small companies and SMEsâĶâ, likening them to successful family-run restaurants that fail when trying to scale-up, Patrowski added that â....we still need big pharma - they talent scout and offer buy-outs, but how can we get everybody to win?â By contrast, a counterpart panel respondent, Kevin Bagley (former Medicaid Director for the State of Nebraska, now at Strategic Consulting) raised the question that âMedicaid covers around 50% of all [US] births, so who will get less moneyâĶ[if we increase cover for orphan drugs]?â, referring to an ongoing debate over resource allocation linked to the rule of rescue. Later, Bagley added that âavailability is not the same as access - we need all sides to bridge the gapâ beckoning collaboration and alliances to improve processes. In short, resolving access issues requires new models and levels of support. On innovation, Bagley went further, boldly stating that âInnovation is at risk! We have gone down a pathway where SMEs push innovation, but then often go out of business. Congress has prioritised innovation but failed to follow throughâ. Here, a careful juxtaposition between urging more state intervention and stepping back to allow free-market freedoms seemed to be at stake - but with little resolution on its conflicts; if ever a space for social science were to be opened!
This sentiment followed in part beyond industry too, and into an âAdvocacy supportâ seminar, with patient organisations questioning âwhether we are competitors or collaboratorsâĶwith undue pressure [from] everybody going for the same pot [of money]â (Frank Rivera, President of Stronger Than Sarcoidosis). The latter saw Josie Godfrey (Co-founder and CEO of Realise Advocacy) - a long-standing mainstay speaker at both World EPA and WODC - and key figure for developing rare disease patient organisations, advised that â...having worked with two patient organisations where people [leaders] would not sit in the same room, it is often better to start small, and work slowlyâ when building collaborations. Thus, a considered and slow approach to community-building is key.
Meanwhile, a few speakers looked to pragmatic concerns the industry faces, in the âPricing and Reimbursementâ panel for example, Marshall Summar (CEO of Uncommon Cures) noted for instance that the US has only around 120 people able to run and/or conduct rare genetic clinical trials, leaving a large skill gap that brings delay to innovation - there are simply too few physicians to meet industry need. Yet few proposed solutions to many of the issues that industry faces. Elsewhere, as keynote Mark Trusheim (Strategic Director of NEWDIGS, at the Center for Biomedical System Design, Tufts Medical Center) proposed that there should be a ârisk-based system where insurersâ licenses could be removed at state level if they fail to provide coverage that has been paid forâ - albeit a position at odds with upcoming changes that allow Medicaid coverage for treatments out of state.
In our own contributions, our team presented research on the value of social media data for diagnosis (Matthew Hanchard) in the âDiagnosisâ panel and a comparison of EU and US orphan drug submissions versus approvals and authorisations (Jin Ding). As a result, we remained largely tied to our respective panels as attendees. But within each panel, and others that we delved into, Jin and I felt that the event and much of its discussion was framed by rapidly shifting policy amidst the run-up to the next US Presidential election, but still firmly steeped in a normative understanding of policy. As such, our presentations - coming from a social science origin - required that we initially justify social science and the value of theory before making our case. As academics, this led us to address a different set of âSo What..?â questions; less on what can this tell us, or why is this significant, and more instead on how does this improve either profit margin or equitable access to healthcare. It will certainly be interesting to trace these debates as they evolve through further conferences in the run-up to the US presidential election, and in the same year as the UK general election and many others across the EU.
- Analysing Gene Therapies: A note on how to find the future
-
by Eva Hilberg and Aleksandra Stelmach

NIC (2020) ''. Available at: https://unsplash.com/photos/gray-laboratory-machine-to8o0bqOA6Q under a CC-BY license.
Gene therapies are undoubtedly the pharmaceutical hot topic of the moment. As the first genuinely revolutionary treatments such as Zolgensma and Libmeldy are slowly being integrated into regular care in several countries, the industry seems to have at last arrived at the often-discussed underlying step-change in the nature of medical treatment, moving to personalised modifications on the molecular level. Gene therapies are cutting-edge techniques that modify âa personâs gene to treat or cure diseaseâ by replacing certain genes with their healthy copies, by inactivating them or by introducing âa new or modified gene into the body to help treat a diseaseâ (FDA 2018). For decades dubbed as the treatments of the future, gene therapies are becoming, as some argue, the treatments of the present, transforming the ways in which diseases, especially rare diseases could be managed and even cured (Finkel 2019). Media reports have turned this new development into âmiracle curesâ (Fay Cortez 2019) promising to treat incurable and rare genetic disorders, giving hope to patients and their families. As more gene therapies are being approved by regulators â in the US for example, the Food and Drug Administration (2023) has so far approved about 30 such novel treatments â the stakes for such types of speculation are increasing, as is the price for each gene treatment (Zolgensma currently has a list price of 1.795 million pounds per dose).
In this context, future visions clearly operate as more than just potentially hyperbolic statements. Instead these (often officially generated) expectations are collectively produced and circulated between actors and within innovation and policy spaces, and they sustain specific agendas and shape policy making (Van Lente 2012). Rather than being mere descriptions of events, expectations have a mobilising and performative function that seek to bring about specific changes to the current situation by emphasising hopes and opportunities rather than challenges and obstacles. In the context of pharmaceutical development, these expectations can also motivate future investment and garner attention for research that is still underway â these types of expectations have in the past been highly pivotal in the development of the modern biotech sector (Cooper 2008). At first glance, the case of gene therapy seems to bring together both the best that research can deliver, and the worst in terms of excess expectation raised on the back of these new developments. We argue that the ways in which futures are at work here can bring about a better understanding of both the way in which pharmaceutical development operates in the post-genomic era, and also how different actors may be positioning themselves at the emergence of a new paradigm of treatment.
A collaborative research project explored these (and other) questions over the past year by beginning to map the promises made and expectations raised during this transition to the future of medical treatment. A team of researchers including Eva Hilberg, Aleksandra Stelmach, Tineke Kleinhout-Vliek, and Paul Martin at the University of 91ÖąēĨ and the University of Utrecht worked together on developing an approach to analysing this emerging vision of the future of medical treatment, and also held an inaugural stakeholder workshop that engaged with the meaning of future narratives for the regulation of new pharmaceuticals. The event mapped different regulatory futures in practical detail, and also began to open the debate to explore a potential for different types of participation, such as NGOs and also government representatives. Overall, it became clear that how the future is envisaged depends largely on who imagines it, and what images and words are used to describe future developments.
These images and words will be studied more closely in the next stages of the project, thus continuing the study of a new field of medical intervention at the moment in which imagination becomes reality. There are of course still numerous challenges to the development of gene therapies, including extremely high prices of treatments that risk undermining the âgene therapy revolutionâ (Editorial 2023) and making it unavailable to patients, especially those from disadvantaged sections of society and from the Global South. The counter-imaginaries already paint the visions of gene therapies as the preserve of the wealthy rather than a cure for the masses (Editorial 2021). The futures of gene therapies as envisioned by patients and their families could also differ significantly from those imagined by companies (see previous blog posts by Jin Ding and Eva Hilberg and Tineke Kleinhout-Vliek). Other key issues remain, such as if gene therapies will work and for how long, and what type of legislation would be needed to make them accessible (Reardon 2023). But the emergence of gene therapy still marks a unique moment of (potential) paradigmatic revolution that could re-set our imagination of future medical treatment for decades to come.
References
Cooper M (2008) Life as surplus: biotechnology and capitalism in the neoliberal era (Seattle: University of Washington Press)
Editorial (2021) Gene therapies should be for all. Nature Medicine, 27 131, https://doi.org/10.1038/s41591-021-01481-9
Editorial (2023). The gene-therapy revolution risks stalling if we donât talk about drug pricing. Nature 616, 629-630. Doi: https://doi.org/10.1038/d41586-023-01389-z
Fay Cortez M (2019) Welcome to the Age of One-Shot Miracle Cures That Can Cost Millionsâ, Bloomberg UK, June 1 available at:
Finkel E (2019). The gene therapy revolution is here. Medicine is scrambling to keep pace. The Conversation June 5. Available at:
Food and Drug Administration [FDA} (2018) What is Gene Therapy?. July 25. Available at: https://www.fda.gov/vaccines-blood-biologics/cellular-gene-therapy-products/what-gene-therapy
Food and Drug Administration [FDA] (2023) Approved Cellular and Gene Therapy Products, June 30. Available at:
Reardon S (2023). âItâs a vote for hopeâ: first gene therapy for muscular dystrophy nears approval, but will it work?, Nature 618, 451-453. doi: https://doi.org/10.1038/d41586-023-01799-z
Van Lente, H. (2012). Navigating foresight in a sea of expectations: lessons from the sociology of expectations. Technology analysis & strategic management, 24(8), 769-782.
- Focus on patientsâ stories
-
Eva Hilberg, PhD
Tineke Kleinhout-Vliek, PhD
21-Jun-2022It looks as though stories are everywhere nowadays. Within qualitative research, there is an increased recognition of the relative power of stories, because we relate to people experiencing things in a different way than we relate to numbers. Stories have a strong affective dimension: you âexperienceâ a story with the person telling it, engaging your emotions as well as your brain. We are also far more likely to remember data in the form of a story. To make sense of our lives, we all engage in story-telling, whether on Instagram or down the pub: about ourselves, our experiences, the people we meet and the things we do. These are, of course, not entirely fictional accounts, but a conscious selection of all the many and muddled âdata pointsâ of life, often with a narrative arc with a clear beginning and an end, and more often than not organized around a problem that is overcome somewhere along the way.
Patients are no different in this, as Arthur Frank so memorably pointed out in the seminal Wounded Storyteller (2nd ed., 2013). Nowadays many patients blog, vlog or even write books to share their diagnostic and treatment journeys with others. They may also get invited to tell their stories at conferences hosted by pharmaceutical companies, or to contribute âlived experienceâ to deliberations on a reimbursement decision on a medicine targeting their illness. From the very first encounter, usually when they first go to their general practitioner, they begin to share their story in a great number of places (Van de Bovenkamp et al., 2020). This is especially the case for rare disease patients, as theirs is often a long road to diagnosis, followed by difficulties in accessing treatment. Along the way, a great many stories then become public property, evoking a strong response from society. One example is baby Jayme, a Spinal Muscular Atrophy patient who, through crowdfunding, got access to treatment with Zolgensma in Hungary, nearly 1,500 km from his home in Rijswijk, the Netherlands (RTL nieuws, 2020).
The increasing focus on patient engagement and involvement also comes from the policy side, with a steadily growing interest in qualitative data. Patientsâ experiential expertise and knowledge are now arguably more valued than they used to be. At the same time, policy makers and regulators are not well-equipped to deal with these more heterogeneous types of information. It is difficult to weigh a patientâs lived experience and personal responses against an incremental cost-effectiveness ratio, which seeks to capture the lived experience of many patients, yet at the same time reduces these to numbers (Mills & Hilberg, 2019) â especially when faced with that particular patient in the decision-making setting (Kleinhout-Vliek et al., 2021).
With so much official emphasis on qualitative experiential data, it is worth bearing in mind that sociology tells us that the setting shapes the input (see for instance overview in Petrakaki et al 2018). Stories are highly contextual, as where you are and whom you meet influences the story you tell, and the result will be interpreted in different ways by each audience. These acts of adjustment and reception occur both on a conscious and subconscious level, all of the time, throughout our lives. This does not mean that the content is less âtrueâ as a result, it only seeks to point out the interpersonal dynamics that go into the representation of individual experience, which can be due to the creation of different expectations, such as for instance those in a diagnostic encounter compared to an official âconferenceâ setting labelled âpatient experienceâ, or a contribution to a board deciding on market access to medicines. The question is, how are patientsâ stories shaped by their setting? What considerations affect this process, which stories are apparently âallowedâ and which not, how are these stories valued (in research and in policy), and what effect may this have on decision-making? In an interdisciplinary strand of research developed in collaboration with Erasmus University Rotterdam, we seek to better understand these matters through observations and key interviews. This matters as it helps us to better conceptualise how social pharmaceutical innovation initiatives are influenced by and shared across a relatively wide variety of settings.
References
Frank, A.W. (2013). The Wounded Storyteller : Body, Illness, and Ethics. Second ed. Chicago, Illinois ; London.
Kleinhout-Vliek, T., De Bont, A., & Boer, B. (2021). Necessity under constructionâsocietal weighing rationality in the appraisal of health care technologies. Health Economics, Policy and Law, 16(4), 457-472.
Mills, C. and Hilberg, E. (2019), âBuilt for expansionâ: the âsocial lifeâ of the WHO's mental health GAP Intervention Guide. Sociol Health Illn, 41: 162-175.
Petrakaki, D., E. Hilberg & J. Waring (2018), âBetween empowerment and self-discipline: Governing patients' conduct through technological self-careâ, in: Social Science and Medicine, Vol. 213, September 2018, pp. 146-153. DOI:
van de Bovenkamp, H. M., Platenkamp, C., & Bal, R. (2020). Understanding patient experiences: The powerful source of written patient stories. Health Expectations: an international journal of public participation in health care and health policy, 23(3), 717.
RTL nieuws (2020). Hoe is het met baby Jayme? 'We hoeven geen afscheid te nemen'. Accessed on 16 June 2022 via https://www.rtlnieuws.nl/nieuws/nederland/artikel/5198170/baby-jayme-spierziekte-sma-behandeling-zolgensma-hongarije - Patient access of orphan drugs in the UK - patient perspectives
-
Jin Ding, PhD
20-Aug-2022What are Orphan Medical Products (OMPs)?
Orphan medical products (OMPs) are used for the diagnosis, prevention or treatment of rare disease, which is defined as a condition affecting fewer than 5 in 10,000 people. Rare diseases can have a severe impact on the quality of life for patients. To date, over 7000 rare diseases have been identified globally, but most of these are without effective treatment. The main factor in this treatment gap for rare diseases is the limited profitability of niche treatments, making it very difficult for pharmaceutical companies to recoup the high costs of drug research and development (R&D) for such small markets.
To better address the unmet medical needs of rare disease patients, regulations have been passed in a number of countries to incentivize the development of OMPs. The US was the first country to pass a dedicated Orphan Drug Act (ODA) in 1983. The EU introduced legislation in 2000, and in 2000 the UK outlined the rules on the application and incentives of OMPs. From 2021, the UK will take over its own national responsibility for products previously governed by EU legislation. Major incentives for stimulating OMPs development include: 7-year market exclusivity, tax credit, fee waiver, research grant and regulatory assistance. On the face of it, these incentives have been a success, as the number of approved orphan drugs has increased since their implementations. To qualify for the incentives, sponsors must submit an application for orphan drug designation to the regulatory agency, for example, the Medicines and Healthcare products Regulatory Agency (MHRA) in the UK.
In the UK, in order to qualify in terms of for a rare condition, a medical product must meet the following criteria:
- It must be intended for the treatment, prevention or diagnosis of a disease that is life-threatening or chronically debilitating
- The prevalence of the condition in Great Britain must not be more than 5 in 10,000, or it must be unlikely that marketing of the medicine would generate sufficient returns to justify the investment needed for its development
- No satisfactory method of diagnosis, prevention or treatment of the condition concerned exists in Great Britain, or, if such a method exists, the medicine must be of significant benefit to those affected by the condition
But it is important to note that not all products used for the diagnosis, prevention, or treatment of rare diseases are OMPs, only medical products authorised by regulatory agencies with an orphan designation can be categorised as OMPs. All and are published on the MHRA website.
Our project
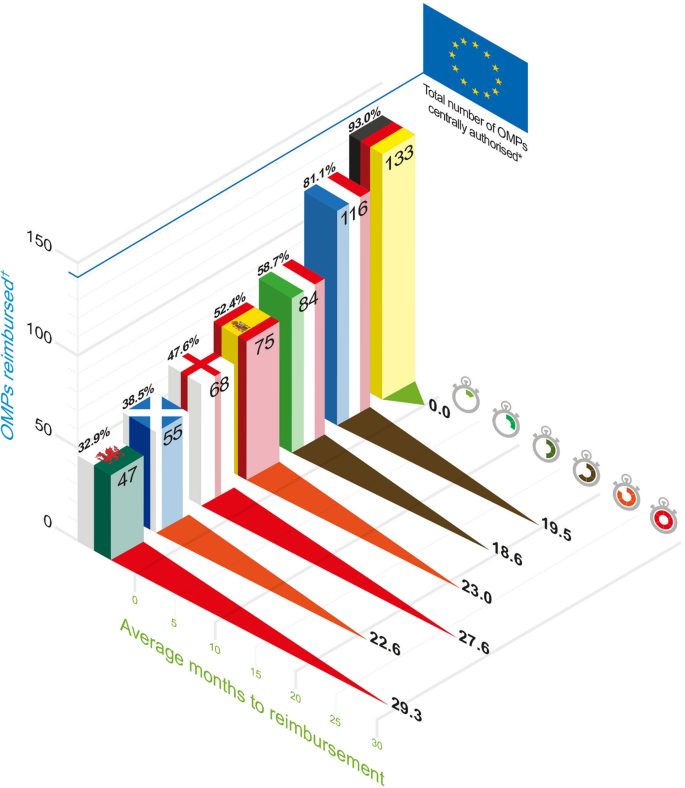
How orphan drug R&D operates in actual practice is far from straightforward. According to our ongoing research as part of a wider analysis of the orphanisation, since the enactment of orphan drug legislation in the EU in 2000 till 2020 (before Brexit), the number of approved OMPs in the EU was only a small fraction of the number of approved OMPs in the US. The gap between the EU and US has been growing since 2010. Once these OMPs have been centrally authorised in the EU, they are assessed on pricing and reimbursement at an individual EU member state (national) level before the drug is made available to patients. The actual accessibility of OMPs varies significantly among EU member states, and in the UK, not all EU-authorized OMPs are in fact recommended by the national health technology assessment agency NICE(The National Institute for Health and Care Excellence). There is also a considerable time delay (27.6 months) between EU authorization and NICE reimbursement decision (see Figure 1).
Figure 1. Comparison of access to OMPs - (from Zomora et al., 2019)
Previous studies about orphan drug accessibility have focused on market access and reimbursement, but they have not taken the perspective of patients into account. Our current project emphasises patientsâ involvement as active and equal participants in this process, seeking to provide an alternative to traditional research approaches in the areas of health economics, health policy, and social sciences.
To recognize the experience, needs, and preferences of rare disease patients without treatments, this participatory research project seeks to answer the following questions:
- Identifying problems: Whatâs the position of UK orphan drug accessibility among the US and major EU countries?
- Assessing impact: What are the implications of inaccessibility for rare diseases patients?
- Informing policy: What are the roadblocks that need to be addressed to improve patient access?
Funding and Acknowledgements
This study is commissioned and funded by Research England.
The first step of this project is to identify the real-life accessibility of orphan drugs, contrasting inaccessibility in one geographical context with those that are available in other countries. Our findings will later be supplemented by further research in order to investigate the impact of the lack of treatments on patientsâ lives. This project is a first step towards this larger analysis, starting with an online survey that will be sent to the UK rare disease patients/patient organisations in October 2022.
We are very keen to work closely with rare disease patient organisations, and look forward to developing long-term collaborative community partnership with UK rare disease patients/patient organisations. If you are interested in this project, would like to take part, or have any questions, please contact us at: orphanisation@sheffield.ac.uk.
Our team
Dr. Jin Ding
Principal Investigator
Dr. Matthew Hanchard Co-Investigator
Dr. Eva Hilberg
Co-Investigator
Prof. Paul Martin
Co-Investigator
Charoula Veneti
Research Assistant
References
Zamora, B., Maignen, F., OâNeill, P. Mestre-Ferrandiz, J., and Garau, M. (2019) 'Comparing access to orphan medicinal products in Europe'. Orphanet Journal of Rare Diseases. 14(95), pp. 2-12.






iHuman
How we understand being âhumanâ differs between disciplines and has changed radically over time. We are living in an age marked by rapid growth in knowledge about the human body and brain, and new technologies with the potential to change them.